Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Meralgia paresthetica [also known as, lateral femoral cutaneous nerve entrapment], is the clinical syndrome of pain and/or neuropathy in the anterolateral thigh associated with compression of the lateral femoral cutaneous nerve [LFCN].
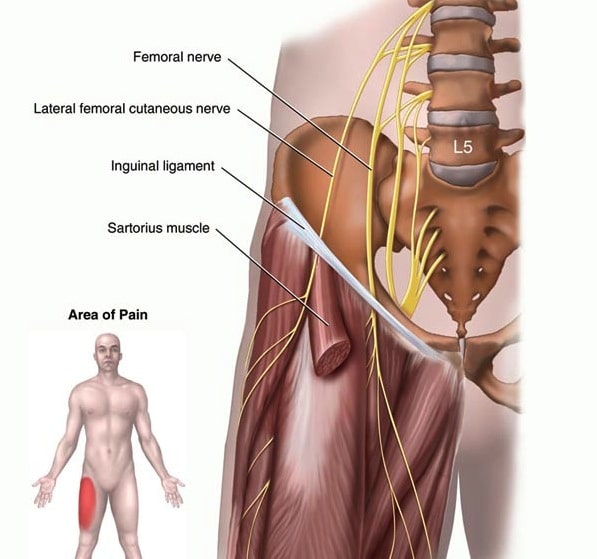
The lateral femoral cutaneous nerve branches off of the lumbar plexus and conveys fibers from the L2 and L3 nerve roots. The nerve courses through the pelvis, running adjacent to the lateral edge of the psoas muscle. It enters the leg underneath or through the inguinal ligament, medial to the anterior superior iliac spine; it is in this location that entrapment can occur.
The lateral femoral cutaneous nerve is a pure sensory nerve that is susceptible to compression as it courses from the lumbar plexus, through the abdominal cavity, under the inguinal ligament, and into the subcutaneous tissue of the thigh.
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Most cases of meralgia paresthetica arise spontaneously and are presumed to result from entrapment of the lateral femoral cutaneous nerve as it passes underneath or through the inguinal ligament.
The most commonly identified risk factors are:
The median age at when patients present with meralgia paresthetica is 50 years.
The incidence is approximately 7 times higher in patients with diabetes compared with the general population.
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Examples related to compression at the inguinal ligament include:
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Meralgia paresthetica is characterized by pain, numbness and tingling (paresthesia), and diminished sensation (hypesthesia) over the upper outer thigh.
Symptoms are usually unilateral and typically the onset of pain is subacute. Patients characterize their symptoms as:
Clinical examination shows a loss of light touch and/or pinprick sensation in a discrete area of the upper lateral thigh, often in a more restricted area than the zone of paresthesias.
Symptoms may be reproduced by tapping over the lateral aspect of the inguinal ligament (Tinel’s sign).
Neurologic findings are limited to sensory changes only, since the lateral femoral cutaneous nerve does not contain motor fibers. Therefore, if physical examination reveals motor deficits (e.g. weakness or abnormal deep tendon reflexes in the affected extremity), then other etiologies should be considered.
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Detailed history must be obtained, especially about recent weight gain, use of tight-fitting clothes or belts, exercise habits, and other potential risk factors for compression at the inguinal ligament. [See ‘Causes and risk factors’ above].
Inquiring history about aggravating factors especially with with Valsalva or prolonged walking is helpful in suggesting inguinal compression.
If pain is present, it should be limited to the anterolateral part of the thigh. Back pain, including radicular pain or “sciatica,” should raise suspicion for lumbosacral spine or plexus pathology rather than meralgia paresthetica.
Neurologic examination:
A focused neurologic examination of the lower extremities must be performed in order to detect diminished sensation in the distribution of the LFCN and also to rule out weakness or reflex changes suggesting an alternative diagnosis.
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
-Clinical Diagnosis
Meralgia paresthetica is a clinical diagnosis based primarily upon all of the following features:
-Imaging
Imaging is generally not necessary if the history and examination findings are characteristic for meralgia paresthetica. Patients with atypical signs or symptoms or an unreliable examination should be imaged to rule out alternative diagnoses.
-Nerve conduction studies (NCS)/electromyography (EMG)
Most patients with typical signs and symptoms of meralgia paresthetica do not require NCS/EMG.
Electrodiagnostic studies can assist in the differential diagnosis and guide the need for imaging of the lumbar spine or pelvis. The role of NCS/EMG is primarily to exclude an L3/L4 radiculopathy, lumbar plexopathy, or femoral neuropathy in patients with atypical clinical presentations.
-Nerve Blockade
Pain relief achieved from anesthetic injection into your thigh where the lateral femoral cutaneous nerve enters into it can confirm that you have meralgia paresthetica. Ultrasound imaging might be used to guide the needle.
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
The differential diagnosis of meralgia paresthetica consists of other peripheral nervous system lesions that supply overlapping sensory territory in the anterior and lateral thigh.
Lumbar Plexus
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Meralgia paresthetica is a self-limited, benign disease in most patients and most patients have spontaneous remission.
Although recurrent symptoms are common approximately more than 90% of patients respond to conservative measures alone.
The acute therapy of meralgia paresthetica includes:
Physical therapy does not play a significant role in the management of this disorder.
In patients with persistent symptoms for more than 1 to 2 months, despite the above measures, reexamining the area to confirm the local nature of the problem is important.
Anticonvulsants such as carbamazepine, phenytoin, or gabapentin may be helpful in reducing neuropathic pain symptoms but have not been systematically studied in meralgia paresthetica.
Tricyclic antidepressants such as amitriptyline may aid in relieving pain.
Consultation with an anesthesiologist for a local nerve block can also be considered for persistent symptoms. Injection of a local anesthetic agent, glucocorticoid, or both can be useful to temporarily treat this neuropathy.
Rarely, surgery is necessary in patients with severe chronic symptoms that are refractory to more conservative measures.
Meralgia Paresthetica Causes, Symptoms, Diagnosis, Treatment
Source: [1],[2],[3],[4]
Recent research has yielded encouraging findings regarding the benefits of these bivalent COVID boosters. However,… Read More
Polycystic ovarian syndrome (PCOS) is one of the most common female endocrine disorders. Polycystic Ovarian… Read More
Around three million Americans suffer from peanut allergies and also tree nut allergies, yet there… Read More
This website uses cookies to ensure you get the best experience on our website.